
Understanding Wound Care: An Overview
As is true of all medical specialties, wound care involves a range of procedures and considerations. Understanding the development, treatment, and documentation of wounds is important in order to effectively support healing and provide optimal patient care.
This article presents an overview of common wound considerations from specialists at Vohra Wound Physicians, the nation’s largest and most trusted wound physician group. Vohra physicians work at over 3,000 skilled nursing facilities across the country and are experts in post-acute wound care.
Wound Development
The wound care specialty focuses on injury and damage to skin and its underlying structures. In order to provide optimal wound care, it is first important to understand how and why wounds develop by considering general anatomic skin layers and pressure ulcer risk factors.
Anatomic Skin Layers
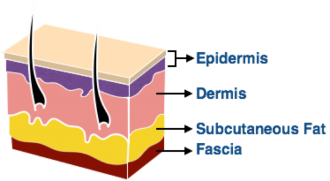
Although the skin has many layers, at its simplest it can be divided into a few topmost portions and underlying structures. The outermost layer of the skin, the epidermis, is the surface layer of the skin. It has a waterproof barrier and minimal blood supply. Directly below it is the dermis, which contains hair follicles, sebaceous glands, blood vessels, and nerve endings.
Below the dermis, there is subcutaneous tissue. This tissue has a lot of fat and serves to cushion the body against outside force, to generate body heat, and to retain moisture. Directly under this is the fascia, which is connective tissue that covers the muscle and holds all internal structures in place. Below the fascia is the muscle itself, followed by the bone.
When a wound is deeper than approximately ¼ inch into the skin, it is considered a deep wound and is far more likely to cause significant damage than a shallow wound.
Pressure Ulcer Risk Factors
One of the most important aspects of wound care, particularly in skilled nursing facilities, is performing an initial clinical assessment of new patients in order to determine their risk for wound development. Risk factors provide particular insight into the likelihood of developing pressure ulcers, or bedsores, which are the most common form of chronic wounds.
According to the Center for Medicare & Medicaid Services (CMS), some of the most common risk factors for pressure ulcer development include:
Impaired/decreased mobility and decreased functional ability
Co-morbid conditions, such as end stage renal disease, thyroid disease or diabetes mellitus
Drugs that may affect healing (e.g., steroids)
Impaired diffusion or localized blood flow (e.g., generalized atherosclerosis or lower extremity arterial insufficiency)
Exposure of skin to urinary and fecal incontinence
Under-nutrition, malnutrition, and dehydration
Presence of a previously healed pressure ulcer
Cognitive impairment
Patient’s refusal of aspects of care and treatment
Understanding a patient’s risk for wounds enables the care team to take appropriate preventative action and to map out a plan of care.
Wound Considerations
When assessing and treating wounds, there are several important considerations. Notable strategies include ensuring proper patient nutrition, avoiding pressure ulcers using pressure offloading, and remaining vigilant for the development of atypical wounds, open wound infections, or geriatric skin conditions.
Nutrition
Quality nutrition is an essential component of successful and efficient wound care. Undernourishment or more severe malnourishment can slow down the healing process.
Consuming foods rich in Vitamin C and zinc can aid in collagen formation and protein synthesis, which are important aspects of wound healing. Since protein is used to build and repair tissues, wound patients should consume a protein-rich diet.
Nutrition can be monitored by weighing patients and performing blood tests, and supplements can be prescribed as needed. If a patient is experiencing unintentional weight loss or has a BMI of below 22, they likely need to increase their food consumption to achieve proper nutrition. For some patients, appetite stimulation may be needed.
The Importance of Pressure Offloading
Pressure ulcers, or bedsores, are a highly common chronic wound that frequently affect elderly patients and those in long-term care facilities. Particularly since they are often avoidable, it is incredibly important that care providers are aware of pressure ulcer prevention strategies. One important way that pressure ulcers can be prevented or addressed is through strategic patient repositioning and the use of support surfaces. This minimizes mechanical load, pressure, and skin friction. When choosing a support surface, it is important to focus on the following considerations:- Pressure redistribution. The goal is to take pressure away from the area where the wound is and redistribute it over a broader or more diverse area.
- Moisture control. Skin that has too much moisture, or is macerated, is prone to breakdown.
- Temperature control. Temperature increases in the skin can impact metabolism. Temperature moderation should be maintained.
- Friction control. Friction can lead to skin weakening and cause pressure ulcers to develop.
Atypical Wounds
Although most wounds fall within the standard wound categories, others are less easy to identify, such as atypical wounds, or wounds of unknown etiology. These wounds typically have uncommon characteristics and either do not heal as expected or quickly worsen. These wounds may be caused by inflammatory diseases, chronic disorders, or certain genetic diseases. A common example of an atypical wound is radiation fibrosis. These occur after radiation treatments for most cancers, pyoderma gangrenosum, pemphigoid, and malignancies. Radiation fibrosis is a late effect of radiation that can manifest as skin induration and thickening, swelling, or tightness. It is caused by the increased formation of collagen and can occur up to several years after radiation treatment. The degree of skin reaction to this treatment is graded on a four-point scale. When treating radiation wounds, it is important to avoid adhesives to the radiation area, as well as bordered gauze and similar materials. These wounds should instead be covered in hydrocolloid and then wrapped in gauze and tape such that the adhesive makes contact with the gauze rather than the wound.Open Wound Infections
When treating wounds, avoiding infection is of significant concern. Infections occur when pathogenic organisms, such as bacteria, invade the wound site and surrounding tissue. The first indicators of infection are pain and wound redness, swelling, and heat. Depending on the severity of the infection, some require medical intervention.
Initially, bacteria can contaminate a wound site without causing infection. Once the bacteria begin to multiply, this is classified as colonization. At a certain point, this colonization begins disrupting wound healing and is considered an infection. Infection leads to inflammation, tissue damage, and a slowed healing response.
Geriatric Skin Conditions
There are several skin conditions that are commonly seen in the geriatric population. Rapid, accurate identification of these conditions can support immediate treatment and ensure patient health. Common conditions to be familiar with include:
- Staph or strep infections: Found on the skin and initially treated with topical antibiotics. Once they invade the surrounding tissue, these should be treated with systemic antibiotics. The specific antibiotic treatment should be determined by performing a tissue culture (swab cultures may not yield the infection-causing organism).
- Impetigo: Pustules with thick crust, sometimes surrounding a blister. Treated with antibiotics.
- Pseudomonas: Best treated with Ciprofoxacin or Cipro. A triple antibiotic solution or Gentamicin can also be applied.
- Anaerobes: The best treatment is to open the abscess so the anaerobe is forced to survive in an aerobic environment, followed by Metronidazole antibiotic.
- Viral infections (e.g., Herpes): Treated with antivirals such as Acyclovir or famciclovir. Sores should be kept covered and treated topically to prevent secondary bacterial infections.
- Warts: Treat with cryotherapy
- Moluscums: Treat with cryotherapy
Video Demonstrations: Draining Abscesses and Chemical Cauterization
One valuable way to improve your understanding of wound care is by observing procedures. Consider two video demonstrations of different types of wound procedures: draining an abscess following infection, and performing chemical cauterization to curb bleeding post-debridement.
These demonstrations are performed by a trained wound care physician for educational purposes. This procedure should not be attempted outside of a care setting with appropriate assessment and oversight by trained medical professionals.
Draining an Abscess
Abscesses can form when wounds are healing from infection. They frequently occur when a superficial skin infection extends into the subcutaneous space and begins to accumulate pus. Without adequate drainage of this area, prescribed antibiotics will not reach the area where the bacteria are growing and the abscess can continue to extend and further propagate the infection.
Draining an abscess can be an effective way of treating a bacterial infection, as they clear the abscess of pus and allow the wound to heal. In the following video, a physician provides a demonstration of abscess drainage.
This demonstration is performed by a trained wound care physician for educational purposes only. A chicken breast model was used in the making of this demo. This should not be tried at home.
Preparing for the Incision
Instruments that may be useful for the incision and drainage of an abscess are a number 15 blade scalpel and a suture removal kit with disposable scissors and forceps. In addition, a local anesthetic such as 1% lidocaine and appropriate syringe and needle will be needed to adequately anesthetize the skin and underlying structures. Before making the incision, the area should be anesthetized and the skin should be cleansed with an anti-microbial agent.
Making the Incision
To begin the draining process, a .5-1cm incision should be made at the pointing or most fluctuant area of the abscess. The fluid and pus will then be expressed from the wound. This incision can be increased as needed to accurately drain the abscess. If needed, a small wick can be placed within the opening to prevent immediate re-closure of the skin as re-epithelialization can occur within 24 hours and the abscess can re-accumulate.
The Necessity of Drainage
Abscesses of long duration often have loculation or multiple pockets within the cavity. These will need to be broken up using a digit or, as is seen in this particular demonstration, using scissors and forceps. To break up these pockets, insert the scissors and spread circumferentially around the abscess cavity to express any remaining pus.
Chemical Cauterization
Chemical cauterization is a valuable way to achieve homeostasis in a wound and to decrease hypergranulation tissue.
In the video below, Dr. Japa Volchok, DO, demonstrates the correct cauterization techniques and discusses the uses of cauterization in promoting wound healing.
This demonstration was performed by a trained wound care physician for educational purposes only and should not be tried at home.
In this video demonstration, chemical cauterization is used to achieve homeostasis in a wound that is bleeding following debridement. Chemical cauterization for hemostasis or treatment of hypergranulation tissue is commonly performed with silver nitrate. Silver nitrate is a chemical caustic agent that is available by prescription. It can sting slightly when applied, so it is important to have adequate anesthesia present in the wound. This can most commonly be achieved with a topical anesthetic.
Silver nitrate application works best when the wound is maximally dried. This can be done by using gauze to apply pressure and dry the wound bed and then quickly removing the gauze and applying the silver nitrate. When silver nitrate is applied, the area will turn black. This can create staining on the skin. If used in areas of visibility such as the face, this should be taken into consideration. Silver nitrate will achieve its hemostatic effect by creating chemical cauterization, or sealing, of the vessels.
In this wound demonstration video, there is a red area at the depth of the wound. This is an oozing vessel. After drying the area, apply the silver nitrate to the area of maximum bleeding. The silver nitrate stick should be rotated gently. As you rotate it, you’ll see that the wound bed has a small gray to black discoloration. This is the silver nitrate that has been left behind. You can also see that the hemostasis has been achieved and that there is no ongoing hemorrhage.
Hypergranulation commonly occurs in a variety of wounds and ulcers, as well as around such surgical wounds as abdominal wounds and feeding tube sites. Without destruction of a portion of the hypergranulation tissue, re-epithelialization cannot occur across the wound. Silver nitrate is commonly used to destroy a portion of the hypergranulation and allow successful wound healing and closure.
Once the silver nitrate has been applied, a wound dressing can then be applied over the wound. The application of silver nitrate as a chemical caustic cauterization agent for treatment of hypergranulation may be required more than once.
Wound Documentation
Appropriate measurement and documentation of wounds is an important facet of proper wound care, as it enables the care team to measure healing progress and provides context for CMS officials during State Surveys.
In the video below, Dr. Japa Volchok, DO, explains how to accurately and consistently measure wounds. He also describes the importance of proper measurement and documentation in the wound healing process.
This demonstration was performed by a trained wound care physician for educational purposes only and should not be tried at home.
Video Description: Measuring and Documenting Wounds
Measurement Tools
For wound measurement, you will want to have a disposable paper or similar measuring device as well as a cotton-tipped applicator. The measuring device is either a paper or plastic disposable measuring tape. It’s generally marked in centimeter markings with sub-markings in millimeters. A cotton-tipped applicator is useful for measuring depth and checking for any undermining.
Measuring the Wound
The model in this video demonstrates a wound. By convention, the superior aspect of the wound would usually coincide with the head. The inferior aspect would be the foot. Length is measured from head to foot. Width is measured from left to right or right to left (the convention does matter in terms of documentation) at the widest part of the wound. Depth is measured at the location with the maximum depth of the wound.
It is important that these measurements are correctly and regularly measured and documented in order to ensure proper analysis of wound healing.
In this instance, Dr. Volchok starts by measuring the wound’s length. The maximum length of this wound is approximately 5.7cm. The width is then measured at its maximum point, which is 2.5cm. The depth is determined by probing the wound with a cotton-tipped applicator. Dr. Volchok probes all areas of the wound to determine the deepest area. It appears to be approximately in the middle of the wound.
After identifying the deepest part of the wound, slide your finger down the cotton-tipped applicator to where it is flush with the intact skin. Pinch the applicator at that point and withdraw from the wound. This can then be laid over your measuring device and the depth determined. In this instance, it appears to be 1.8 or 1.9cm.
Checking for Undermining
Once the length, width, and depth of the wound have been measured, it is important to then record any evidence of undermining. Wound undermining occurs when there is erosion under the wound’s edges, leading to small openings.
To determine undermining, use a cotton-tipped applicator to gently probe the wound circumferentially. In areas with undermining, the cotton-tipped applicator will slip deeper under the wound. The area where the applicator slips the deepest is the maximum area of undermining and should be documented. Measure the depth of undermining in the same way that you measure the depth of the wound.
By convention, the superior aspect of the wound, or the head aspect of the wound, represents 12 o’clock. If we then progress clockwise around a clock face, the area of maximum undermining can be recorded at the consequent time location. In this video, the undermining is approximately 1.7cm deep at 10 o’clock.
Documenting Non-Healing or Slow-Healing Wounds
When a patient’s wound is slow-healing or non-healing for an unknown reason, consistent documentation is critical. Your records should, at the minimum, include a measurement of the wound’s length, width, depth, tissue type, exudate, odor, and periwound description. The width, length, depth, exudate and tissue type are particularly important to document because they’re used in calculation of a Pressure Ulcer Scale for Healing (PUSH) score.
Determining Necessary Measurements
Sometimes necessary measurements are determined by the local coverage determination. For the assessment of wounds and for the payment of wound care services, almost all coverage providers require at least documentation of wound dimensions, drainage, inflammation, swelling, pain, and the presence or absence of necrosis.
Navigating Wound Regulations at Skilled Nursing Facilities
The Center for Medicare & Medicaid Services (CMS) has federal guidelines on wound healing and treatment. CMS surveyors adhere to these guidelines when inspecting and assessing the quality of care at skilled nursing facilities (SNFs) across the United States, and these regulatory criteria help to determine whether or not the facility is at fault when a patient develops a new wound or when an existing wound worsens.
As a result, it is crucial that nurses and healthcare staff who work in skilled nursing facilities have a firm understanding of the criteria that CMS surveyors use to determine whether or not a patient is receiving the appropriate preventive care and treatment for their wounds.
Nurses at SNFs should understand how these guidelines are defined by the regulating body for several reasons:
To increase the quality of care for patients
To be able to advocate on behalf of the facility and their own care practices when necessary
To ensure the patient is indeed receiving the proper care by at least meeting the minimum guidelines set forth by CMS and, subsequently, to be able to communicate those efforts to the CMS surveyor
To provide transparency around wound care practices at the facility
To ensure that nurses and staff are implementing correct and consistent interventions, particularly for patients whose wounds are considered unavoidable
To decrease the likelihood of receiving a citation or disciplinary action
Avoidable and Unavoidable Wounds
One important component of effective CMS adherence is understanding avoidable and unavoidable wound classifications. In the F-686 Guidelines, CMS outlines a list of criteria in order to determine whether a patient’s wound was an unavoidable occurrence and would have happened regardless of the care they received.
CMS defines an unavoidable pressure wound at a skilled nursing facility as a wound that has developed in a patient even though the facility properly evaluated the patient’s risk factors, implemented and monitored the appropriate interventions, and adjusted the care plan according to the patient’s evolving condition. Wounds are classified as avoidable if the facility failed to take any of these actions and a wound developed or worsened.
If a wound is determined to be unavoidable by the surveyor, the facility and care team will not receive a citation. It cannot be understated that even unavoidable wounds still require consistent intervention and treatment to improve patient outcomes. If the surveyor determines that the wound could have been avoided had the proper wound care procedures been followed, a citation will be issued.
Conclusion
Wound care is a nuanced specialty that requires in-depth understanding of wound development, wound care considerations and documentation, and CMS regulatory oversight. The information presented in this article aims to provide general knowledge of these topics and raise awareness of the wound care practice.
To increase awareness of other important wound care considerations, Vohra Wound Physicians has helped thousands of clinicians earn the Vohra Wound Certified Nurse (VCWN™) credential through our Wound Care Certification Program. This program includes 14 modules on effective wound care, with topics including Acute & Chronic Wounds, Atypical Wounds, Preventing Rehospitalization, and Pressure Injuries.
Vohra Wound Physicians is the nation’s most trusted wound care solution. Founded in 2000, Vohra works with nearly 3,000 skilled nursing facilities and uses innovative, proprietary methodologies and technologies to provide superior wound healing to patients.




Stay up to date on the latest in wound care.
Join our mailing list today!



Thank You For Successfully Registering!
Stay tuned for the latest news and treatments in wound care tailored for medical professionals like you.


