


Diabetic Foot Ulcer – Causes, Treatment, and Prevention


What is a Diabetic Foot Ulcer?
Causes of Diabetic Foot Ulcers
Symptoms of Diabetic Foot Ulcers
DFUs are usually diagnosed by visual inspection, sometimes prompted by pain. Patients with neuropathy may not know that they have a wound at all unless they see exudate on their socks or develop an infection.
People with diabetes should examine their feet daily, using a mirror to see the plantar surface if necessary. Annual clinical exams by a healthcare provider are also an excellent way to pick up on ulcers that may have escaped notice.
Classification of Diabetic Foot Ulcers

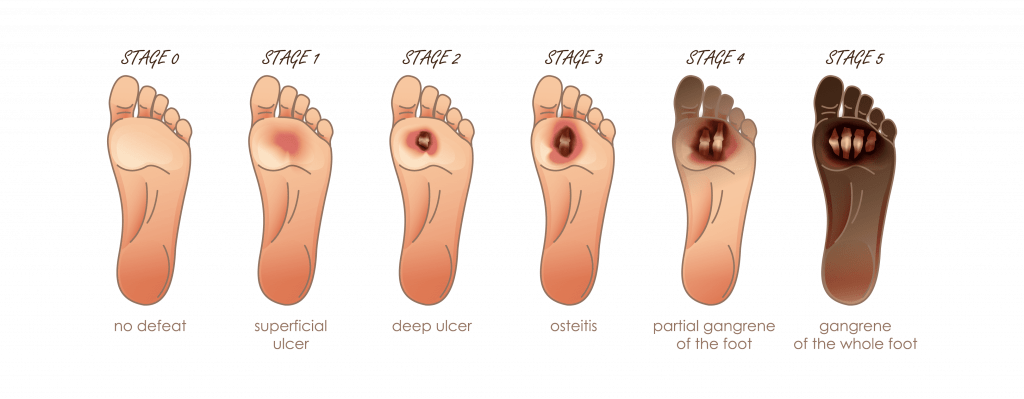
There are a few classification systems for DFUs. The first and most commonly used is the Meggitt-Wagner ulcer classification. This identifies five grades of ulcers:
- At risk, healed ulcer, bony deformities.
- Superficial ulcer with no subcutaneous tissue exposed.
- Penetration through tissue including subcutaneous tissue, bone, tendon, ligament, or joint capsule.
- Infections (osteomyelitis, abscess).
- Gangrene of digit.
- Gangrene of the foot.
This system has limited clinical utility as it does not address some important wound variables.
The American Diabetes Association (ADA) moved away from classification and developed a more clinically relevant consensus recommendation about assessment. This includes evaluating trauma, duration, progression (improving or deteriorating), prior treatment, signs of ischemia, signs of infection, depth, and wound appearance.
How to Evaluate a Diabetic Foot Ulcer
- Primary forefoot, which includes toe deformities and abnormalities of the metatarsal bones.
- Primary midfoot; flat foot deformity, hyper pronation with hindfoot valgus, Cavus foot, and vertical talus.
- Primary hindfoot; varus heel, valgus heel, equinus deformity
- Compound. This refers to Charcot and club foot deformities.
- Patients with Charcot deformity often develop wounds in the central “rocker bottom” area.
Clinical Assessment
- Wounds on the plantar foot
may have callus around the periphery. There is frequently a fibrous quality to the tissue overall. In severe
cases, joint capsules, bones, tendons, muscles, and/or ligaments may be visible in the base of the wound.
Wound assessment should include:
- Measurement of length, width, depth, and any undermining or tunneling present.
- Tissue type – granulation, necrosis, eschar, slough.
- Drainage quality, quantity.
- Periwound appearance.
- Any odor or other concerning findings.
- Arterial adequacy should
be assessed initially by palpating the dorsalis pedis and posterior tibialis pulses. If the pulses are weak
or absent, additional studies should be performed.
- Arterial duplex with ankle brachial indices (may be artificially elevated). This is the typical first step in evaluating the degree of arterial insufficiency.
- Toe pressure readings
- The following studies may be
part of the evaluation of potential surgical candidates.
- Transcutaneous oxygen tension (TcPO2)
- MRA (magnetic resonance angiography)
- CTA (computer tomography angiography)
- Angiogram
- Neurologic status must
also be assessed to gauge the presence or degree of neuropathy contributing to delayed healing.
- Monofilament testing or vibration perception testing is very helpful in diagnosing neuropathy.
- Hot-cold perception and Achilles deep tendon reflex may provide additional information. Patients with neuropathy do not have adequate protective sensation and are at increased risk of wound development.
How to Treat Diabetic Foot Ulcers
Diabetic foot ulcers require standard wound care as well as management of contributing factors, including:
- Pressure reduction. Appropriately fitted footwear can be of great benefit in offloading wounds in an ambulatory patient.
- Debridement to keep the wound clean and free of necrotic tissue. The ADA recommends performing debridement “early and often” for DFUs.
- Moist wound healing. Dressing materials should be selected by the appearance of the wound and the amount of drainage present. The goal is to keep the wound bed moist, not allowing it to dry out nor to become macerated and over-saturated with fluid.
- Advanced wound care products such as growth factors and skin substitutes may be effective.
- Hyperbaric oxygen therapy may be beneficial in some cases.
- Vascular disease. It is important to assess arterial adequacy, as above. Physicians should have a low threshold for further evaluation and referral to a vascular surgeon for procedures to improve blood flow.
- Neuropathy. Patients with inadequate protective sensation must have appropriately fitted protective footwear that offloads the wound and protects from further injury. Patient education is very important to help the patient manage their feet.
- Infection. Given the increased incidence of infection, physicians should have a high level of suspicion of infection in DFUs that deteriorate. The usual signs and symptoms of infection may not be obvious in an infected DFU due to the decreased immune response. Osteomyelitis may present simply as a stalled wound with few other clinical findings.
Long-term Management and Prevention of Diabetic Foot Ulcers
- Multidisciplinary care is very beneficial for diabetics. Studies have shown a 50-75% decrease in amputation rate for patients treated in multidisciplinary diabetic clinics.
- Diabetic foot clinics may include specialists in:
- Endocrinology
- Podiatry
- Vascular surgery
- Physiatry/physical medicine
- Physical therapy
- Nutrition
- Management focuses not just on the wound, but on the patient’s health status and glucose management overall. Education plays an important role in reducing risk and preventing wounds.
Conclusion
FAQs
What does a diabetic ulcer on foot look like?
Ulcers are a break in the skin, typically with pink or yellowish tissue in the base. There may be a buildup of callus around the edges of the wound and it may be quite deep. Infected wounds are often erythematous and may be painful, swollen, and have significant amounts of drainage (which may be purulent).
How serious is a diabetic foot ulcer?
Diabetic foot ulcers are a very serious health problem. The incidence of infection, which may be life-threatening or lead to amputation, is much higher than in non-diabetic ulcers. Additionally, patients who have had a DFU are at increased risk of developing additional wounds.
How long does a DFU last?
It is difficult to predict time-to-heal for diabetic foot wounds. Approximately 75% of patients with foot ulcers are referred for specialty wound care more than a month after onset and may have been caring for the wound at home for far longer than this. Additionally, wound infection and vascular compromise significantly delay healing, if they are present. For a non-infected wound with good circulation and early wound care, the wound may heal in 2-3 months. More complicated wounds may last much longer and require surgical intervention to heal.
Are there home remedies for DFUs?
Diabetic patients who develop wounds should see their physician for treatment. Given the risk of infection and limb loss, early intervention can be critical. Steps that can be taken at home while being treated by a physician include making sure that the area is offloaded with appropriate footwear. Avoid ongoing rubbing or trauma. Do not soak the foot or use toxic cleansers or home remedies in the wound itself. Patients should maintain euglycemia as much as possible and quit smoking if they smoke (as it contributes to arterial compromise).
What helps diabetic wounds heal faster?
See a physician for wound management and follow their treatment plan, including any recommended
studies or referrals.Do everything possible to obtain good glucose control
Protect the feet from trauma with appropriate footwear.
Do not walk on the wound.
Elevate the feet off the floor when sitting.
Keep the area clean, and wear clean socks daily (if the dressing allows).
Should diabetic foot ulcers be covered?
Open wounds heal best when appropriate wound care is used. This includes the use of products and dressings designed to promote a moist environment that facilitates healing. Leaving ulcers open to air may increase the risk of infection, slow the healing process, and soil socks and shoes with drainage.
Resources and References
- The current burden of diabetic foot disease, J Clin Orthop Trauma. 2021 Jun; 17: 88–93. Published online 2021 Feb 8. doi: 10.1016/j.jcot.2021.01.017
- Decreasing incidence of Major Amputation in Diabetic Patients: A Consequence of a Multidisciplinary Foot Care Team Approach. Diabetic Medicine 12 (9): 770-76, Sept 1995
- PLoS One. 2017; 12(5): e0177176
- American Diabetes Association: Clinical Practice Recommendations: Diabetes Care, 21(suppl 1): 1999.
- Published online 2017 May 12. doi: 10.1371/journal.pone.0177176
- Severity and duration of diabetic foot ulcer (DFU) before seeking care as predictors of healing time: A retrospective cohort study
Hilde Smith-Strøm,1,2,* Marjolein M. Iversen,1,3 Jannicke Igland,1,2 Truls Østbye,4 Marit Graue,1 Svein Skeie,5 Bei Wu,6,7and Berit Rokne1